Clinical Diagnostic Parasitology Laboratory (CDPL)
Parasite serology
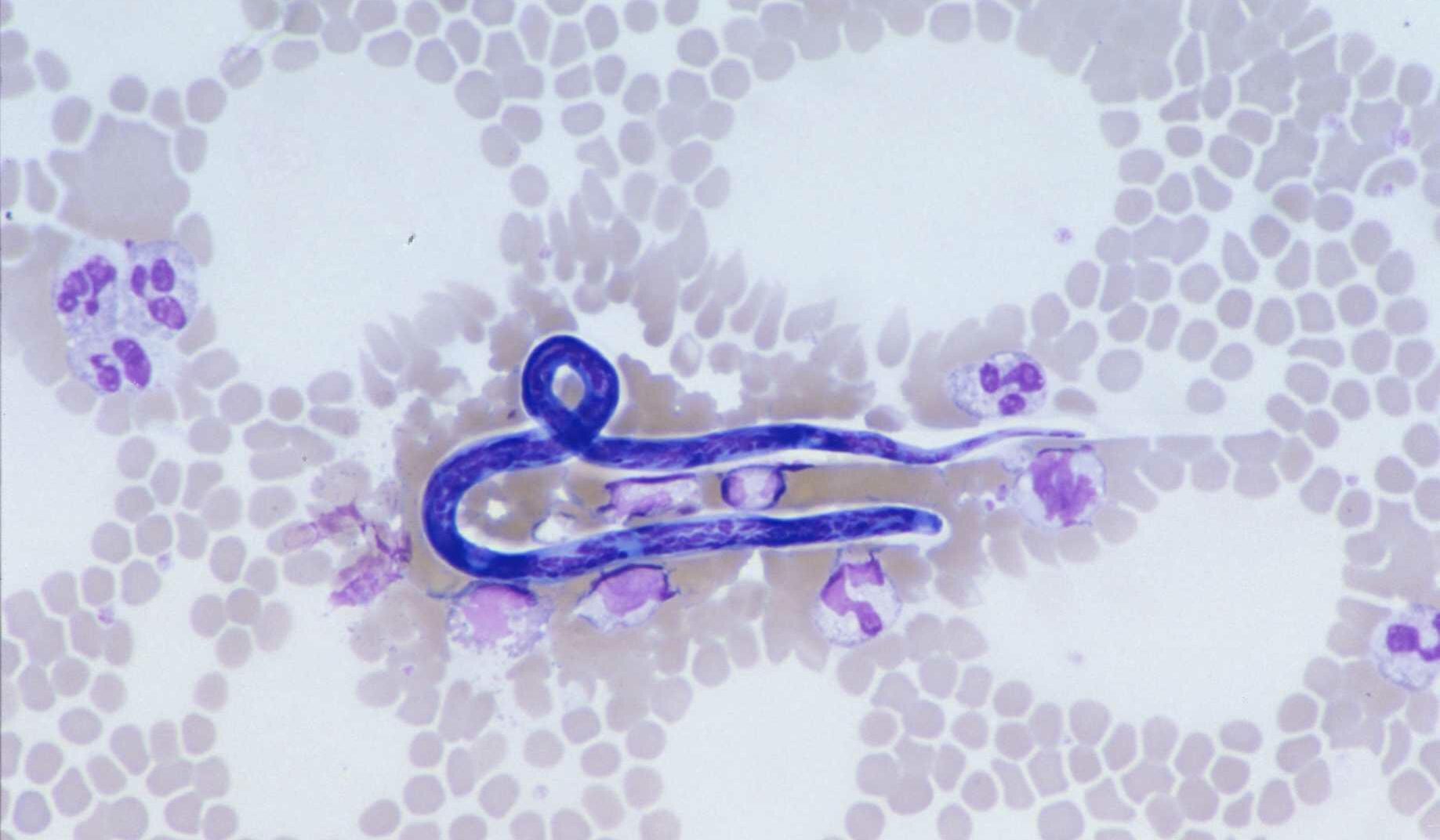
Filaria
Filariasis – UKAS accredited test
Commercial ELISA used. This utilises Acanthocheilonema viteae antigen, that will cross-react with human filariasis species, and detects IgG antibodies.
Antibody levels detected around two to three months post-exposure.
Antibody levels negative from one year or longer after successful treatment.
| SENSITIVITY % | SPECIFICITY % | |
| ELISA (in house verification) | 100 | 90 |
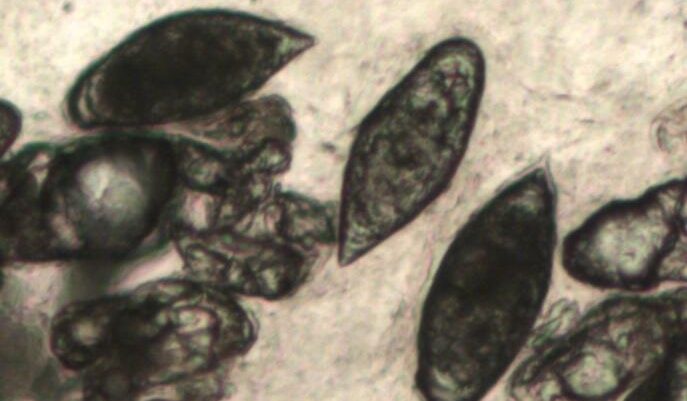
Schistosomiasis
Schistosomiasis – UKAS accredited test
Commercial ELISA used. The test utilises Schistosoma mansoni antigen, however, this does cross-react with other Schistosoma species. IgG antibodies are detected.
| SENSITIVITY % | SPECIFICITY % | |
| ELISA (in house verification) | 100 | 60 |
Antibody levels may not be detected until three months post-exposure.
In patients with a negative ELISA test up to three months but with significant freshwater exposure, we would recommend further testing from four months after the last exposure.
Antibody levels may be positive for 18 months or longer after successful treatment.
Strongyloides
Strongyloidiasis – UKAS accredited test
Commercial ELISA used. IgG antibodies are detected.
Cross-reactions are known to occur in patients with filarial infections and with heavy Hookworm infections.
HIV status has no effect on Strongyloides antibody test
Antibody levels normally detected two to three months post-exposure, however, there are occasions when no antibody response will be detected.
Antibody levels revert to negative approximately six months to one year after successful treatment.
| SENSITIVITY % | SPECIFICITY % | |
| ELISA (in house verification) | 95 | 95 |

Strongyloides
Hydatid (Echinococcus granulosus) – UKAS accredited test
Samples are screened with commercial ELISA. IHA is performed on ELISA positive samples.
Among proven cases of hydatid disease, 92% show a positive ELISA test.
Sensitivity depends on cyst site: Liver 96%, pulmonary 76%, skeletal 60%, other sites vary. Brain hydatid rarely shows positive serology. Serological cross-reactions, giving rise to false positives, can occur with other parasitic infections, particularly larval cestodes and filarial worms and with some neoplasms. Less than 3% of non-infected controls are positive.
False negatives may occur (about 8%) and are more common in patients with extra-hepatic cysts. False negatives can be due to calcified cysts. Patients with cysts occurring in the brain are usually serologically negative.
Antibody levels are detected at variable timescales post-infection due to the nature of the disease.
Antibody levels may remain positive for life after successful treatment/surgery.
IHA is performed on all samples with positive hydatid ELISA serology.
| SENSITVITY % | SPECIFICITY % | |
| ELISA (in house verification) | 100 | 97.6 |
| IHA (manufacturers analysis) | 93 | 94.9 |
The sensitivity of the ELISA is estimated to be 97%. Cases with negative serology but subsequently proven hydatid disease have mainly been in patients with extra-hepatic lesions.
Samples found equivocal by ELISA are re-tested by IHA. We consider the results significant if both tests are positive. If the sample shows equivocal results, we would suggest repeating serology in one month.
ELISA utilises Echinococcus species antigen and detects IgG antibodies.
IHA uses Echinococcus granulosis antigen.

Amoebiasis – entamoeba histolytica
Amoebiasis (Amoebic Liver abscess) – UKAS accredited test
IFA used as an initial screen. Urgent or positive IFA samples will have a secondary test performed. Up to 95% of Amoebic liver abscess (ALA) patients are seropositive by two weeks post-infection. Lower level positive results may be obtained if tested earlier than two weeks post-infection. In these cases, a low-level positive result may be significant and a repeat test should be performed at 14 days’ post-infection. Titre will decrease in one to two months after successful treatment but may remain low level positive for an extended time.
Entamoeba histolytica antigen used. IgG antibodies detected.
| SENSITIVITY % | SPECIFICITY % | |
| IFA AMOEBIASIS | 93.8 | 96 |
| SECONDARY TEST (in house verification) | 100 | 91.6 |

Malaria
IFA used.
If current infection is suspected blood films must be examined. Antibody testing may be useful for retrospective diagnosis.
Antibodies are detected about seven to 15 days from the initial infection.
In a non-immune traveller is treated for a single infection, Ab levels should fall within three to six months of successful treatment.
Plasmodium falciparum and Plasmodium vivax antigens are available, however, species are known to cross-react. Plasmodium falciparum antigen is used unless otherwise requested. IgG antibodies detected.

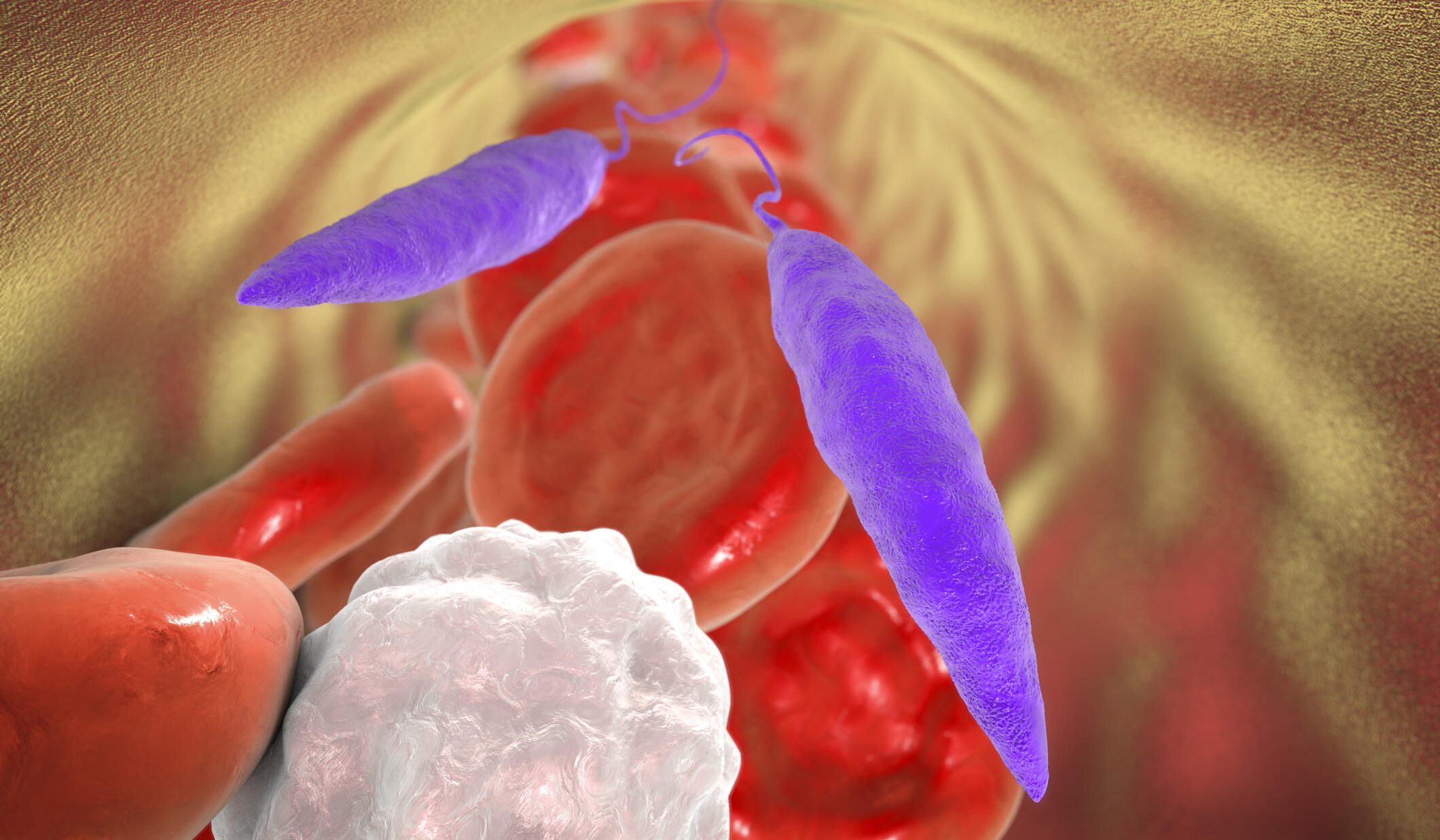
Leishmania
IFA used plus commercial Leishmania dipstick in non-cutaneous queries.
Ab levels detected around one month post-exposure.
The IFA should seroconvert to negative within six to nine months of successful treatment.
Antibody detection is useful in cases of suspected Visceral Leishmaniasis who do not have HIV infection. In suspected Visceral Leishmaniasis patients who are HIV infected sera is often non-reactive.
In Cutaneous Leishmaniasis, serology is of little value.
Cross-reactions may occur with trypanosomiasis and autoimmune conditions.
| SENSITIVITY % | SPECIFICITY % | |
| LEISHMANIA IFA | 94 | 94 |
| LEISHMANIA DIPSTICK (in house verification) | 75 | 100 |
IFA uses Leishmania donovani antigen. IgG antibodies detected. Secondary dipstick detects rK39 antigen.
Fasciola
Fasciola – UKAS accredited test
Commercial ELISA used. This utilises Fasciola species antigen and detects IgG antibodies.
Antibody levels detected around two to three months post-exposure.
Antibody levels should revert to negative around six months after successful treatment.
| SENSITIVITY % | SPECIFICITY % | |
| ELISA (In house verification) | 100 | 77 |
African trypanosomiasis
IFA used for T.b.rhodesiense queries. IgG antibodies detected.
CATT used for T.b.gambiense queries:
- In-house verification SENSITIVITY 100%
- In-house verification SPECIFICITY 98%
Travel history and clinical details are required to determine which test is performed.
Cross-reactions may occur between trypanosome and leishmania serology.
CSF samples can also be tested for African trypanosomiasis antibodies.
South American trypanosoma Cruzi
South American T.cruzi – UKAS accredited test
Serology is useful. Abs are detected around one month post-infection and remain positive for life.
Commercial T.cruzi test used.
| SENSITIVITY % | SPECIFICITY % | |
| in house verification | 100 | 100 |
Positive results are always repeated for quality purposes, first at LSTM, then repeated at another site.
